|
| Liver diseases and their clinical manifestations can only be understood through a sound knowledge of the normal structure and function of the liver. For example, an understanding of the anatomy of the biliary tract, from canaliculus to common bile duct, is necessary to comprehend the basis and sequelae of obstructive jaundice. On the other hand, some liver disorders and their manifestations can only be understood in the context of the functional complexity of the liver. |
|---|
|
The histology of the liver is usually described on the basis of smaller units, called liver lobules. The most common description is that of the classic liver lobule, which consists of a number of liver cells (hepatocytes) surrounded by connective tissue. Such a liver lobule is usually hexagonal, with a central vein in the middle. The liver cells are arranged in plates with blood filled spaces, the sinusoids, in between the various plates of cells. At many of the corners of these hexagonal lobules, triads are found. Each consist of a bile duct, vein (branch of portal vein), and artery (branch of hepatic artery).
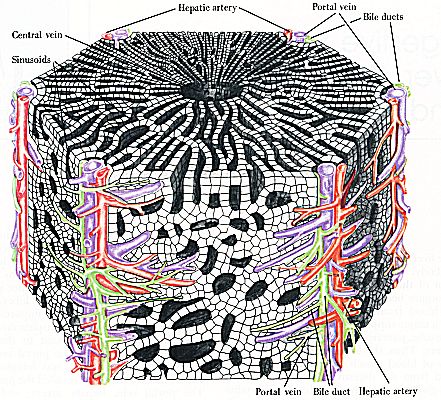
Fig RR472-01 Ross and Romrell p. 472 |
|
The following slide is of a cross section of the liver. Pig liver has more pronounced connective tissue septae and is used here to demonstrate the septae.

Fig 68-001 |
|
Other models to describe a liver lobule are also available.
Classic lobule
Fig RR481-01 Ross and Rommell p. 481 |
|
A portal lobule has a bile duct, in the triad, as its centre. This lobule is triangular.
Portal lobule
Fig RR481-02 Ross and Rommell p. 481 |
|
A liver acinus is described on grounds of the blood supply. Here the branches of arteries from the triads, running on the sides of the hepatic lobule, form the centre of the lobule. This lobule is oval and can be further divided into three zones. Zone one will be closest to the artery, and zone three the furthest (thus the closest to the central vein). When ischaemia occurs, the cells furthest from the blood supply (zone 3) will be most vulnerable, causing centrilobular necrosis.
Liver acinus
Fig RR481-03 Ross and Rommell p. 481 |
|
This is a cross section of a liver of a patient who died of liver cirrhosis. The centrilobular cells were spared, but those closer to the connective tissue septae died. The type of pathology thus determines which model of liver lobules is most applicable.
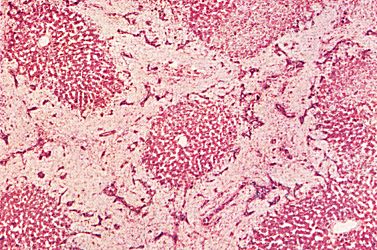
Fig Curran20-01 Curran p. 20 |
|
Each portal tract or triad consists of a bile duct, artery and vein. Sometimes more than one artery or vein may be present. A single layer of cuboidal epithelium lines the bile duct.
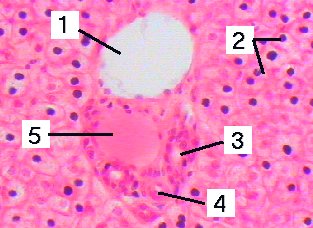
Fig 46-001 |
| On larger magnification, the detail of the hepatocytes and sinusoids
can be seen.
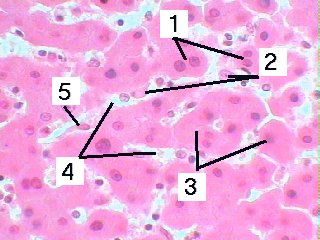
Fig 46-002 |
|
On electron microscopic level it can be seen that each sinusoid is lined by endothelial cells and Kupffer cells (derived from monocytes), and that a space is formed between the endothelial cells and liver cells. This perisinusoidal space of Disse is filled by plasma that leaks through from the sinusoids. Here the liver cells come in direct contact with the plasma.
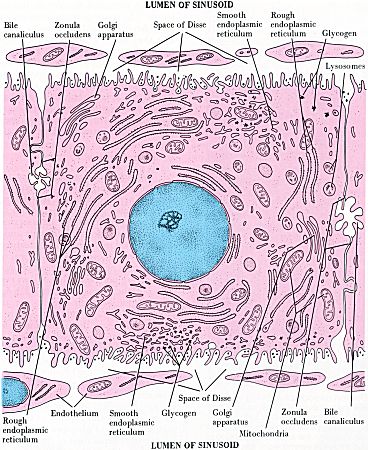
Fig RR476-01 Ross and Romrell p. 476 |
| Reticular fibres are abundant in the space of Disse, and these can
be seen in the following specially stained slide.
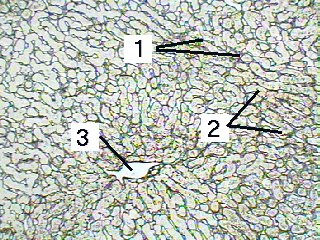
Fig 48-001 |
|
The blood supply of the liver is complicated and summarized in the following diagram:

|
|
It should be remembered that the sinusoids thus contain a mixture of arterial (25%, coming from hepatic artery) and venous (75%, coming from portal vein) blood. A graphic representation of the blood flow is shown below.
Fig TG779-02 Tortora and Grabowski p. 779 |
|
In this figure, biliary flow, going in the opposite direction that blood flow, is also shown. The bile canaliculi open into the interlobular bile ducts, which join to form larger bile ducts.
Fig TG779-01 Tortora and Grabowski p. 779 |
| When the liver is injected with Berlin blue, the sinusoids and central
vein are stained with the blue dye.
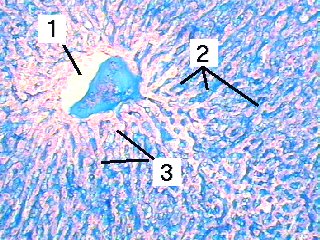
Figure 110-001 |
| Liver |
Slides 68 |
||
|---|---|---|---|
| Fig 68-001 | Fig 46-001 | Fig 46-002 | |
| Fig 110-001 | Fig 48-001 | ||
| Memorandum | ||
|---|---|---|
| References | Fig 68-001 | Fig 46-001 |
| Fig 46-002 | Fig 48-001 | Fig 110-001 |
![]()